

Key Takeaways
- Total knee arthroplasty (TKA) is one of the most performed elective surgeries in the United States, with procedure volume projected to grow to nearly 3.5 million annually by 2030 (Konnyu et al., 2023a).
- Prehabilitation before TKA reduces complication rates and improves strength, function, and quality of life, with effects strongest in the first 6 months after surgery (Konnyu et al., 2023b).
- Physical therapy is the cornerstone of knee replacement rehabilitation, with resistance training significantly improving pain, muscle strength, and function post-TKA (Lim & Kim, 2025; Wei et al., 2024).
- Occupational therapy is essential after TKA, addressing ADL performance, adaptive equipment, home safety, and return to meaningful activities (Kim et al., 2026).
- Telerehabilitation after TKA is as effective as in-person rehabilitation, with equivalent pain and functional outcomes and significantly lower hospital resource utilization (Tsang et al., 2024).
- Outpatient and home-based rehabilitation produce equivalent outcomes after knee arthroplasty, allowing individualized rehabilitation planning based on patient access and preference (Zhao et al., 2023).
 Important: The information on this page is educational only and is not a substitute for individualized surgical or rehabilitation advice. Knee replacement rehabilitation protocols vary based on surgical approach, implant type, surgeon preference, and individual patient factors. Always follow the specific precautions and rehabilitation plan provided by your surgeon and therapy team.
Important: The information on this page is educational only and is not a substitute for individualized surgical or rehabilitation advice. Knee replacement rehabilitation protocols vary based on surgical approach, implant type, surgeon preference, and individual patient factors. Always follow the specific precautions and rehabilitation plan provided by your surgeon and therapy team.Contents
- What Is Knee Replacement?
- Who Needs Knee Replacement?
- Types of Knee Replacement Surgery
- Prehabilitation: Getting Ready for Surgery
- Who Provides Knee Replacement Rehabilitation?
- Occupational Therapy After Knee Replacement
- Physical Therapy After Knee Replacement
- Telerehabilitation After Knee Replacement
- What to Expect During Recovery
- References
1. What Is Knee Replacement?
Total knee arthroplasty (TKA), commonly called knee replacement, is a surgical procedure in which damaged cartilage and bone in the knee joint are removed and replaced with artificial implant components that replicate the smooth, gliding surfaces of a healthy knee (Konnyu et al., 2023a). The procedure relieves severe pain,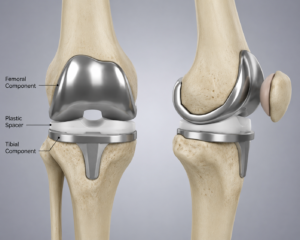 restores mobility, and significantly improves quality of life in people with end-stage knee disease.
restores mobility, and significantly improves quality of life in people with end-stage knee disease.
Knee replacement is among the most frequently performed elective surgical procedures in the United States. Procedure volume is projected to grow to nearly 3.5 million annually by 2030, driven by an aging population and rising prevalence of knee osteoarthritis — with the greatest growth occurring in patients under 65 years of age (Konnyu et al., 2023a). Despite being highly successful, between 10% and 30% of patients report suboptimal outcomes after TKA, making skilled rehabilitation essential to achieving the best possible result (Konnyu et al., 2023b).
Rehabilitation after knee replacement requires a coordinated team effort. Physical therapists lead exercise-based recovery, occupational therapists address daily living function and home safety, and speech-language pathologists contribute when cognitive or communication factors affect rehabilitation participation. Together, this multidisciplinary approach drives both short-term and long-term outcomes (Konnyu et al., 2023a; Kim et al., 2026).
 For Patients and Families
For Patients and Families
- Knee replacement is one of the most common and successful elective surgeries performed — and rehabilitation is what determines how well and how quickly you recover (Konnyu et al., 2023a).
- Between 10% and 30% of people report outcomes below their expectations after TKA — early, consistent engagement in PT and OT significantly reduces that risk (Konnyu et al., 2023b).
- The surgery removes pain from a worn-out joint, but the muscles around the knee still need to be rebuilt through exercise and rehabilitation — this takes months, not weeks (Lim & Kim, 2025).
 For Clinicians
For Clinicians
- TKA is one of the highest-volume elective surgical procedures in healthcare, with 650,000+ performed annually in the US, projected to reach 3.5 million by 2030 (Konnyu et al., 2023a).
- A systematic review of 53 RCTs found that various post-TKA rehabilitation programs produce comparable improvements in pain, range of motion, and ADLs — supporting individualized, patient-centered rehabilitation planning (Konnyu et al., 2023a).
- Between 10–30% of TKA patients report suboptimal outcomes; identifying and targeting at-risk patients for enhanced prehabilitation and rehabilitation is a clinical priority (Konnyu et al., 2023b).
2. Who Needs Knee Replacement?
Knee replacement is recommended for people with severe knee pain and functional limitation that has not responded adequately to conservative management, including physical therapy, medications, activity modification, weight management, and injections. The most common reason for TKA is osteoarthritis, which causes progressive cartilage loss, bone-on-bone pain, stiffness, and loss of function that significantly limits daily activities and quality of life (Konnyu et al., 2023a). For more on OA management before surgery becomes necessary, see the Osteoarthritis page.
Other reasons for knee replacement include rheumatoid arthritis, post-traumatic arthritis from prior knee injury or fracture, and other conditions that destroy joint cartilage. Knee replacement is typically considered when pain is severe and constant, significantly limiting walking, stair climbing, rising from a chair, and sleep. The decision is made jointly by the patient and their orthopaedic surgeon based on symptoms, imaging findings, and overall health (Konnyu et al., 2023a).
People with neurological conditions such as multiple sclerosis, Parkinson’s disease, or stroke history who require knee replacement present additional rehabilitation complexity. OT and PT play heightened roles in these populations, integrating knee replacement recovery with management of the underlying neurological condition (Konnyu et al., 2023a; Kim et al., 2026).
For Patients and Families
- Knee replacement is typically recommended after conservative treatments — including physical therapy, medications, and injections — have been tried and are no longer providing adequate relief (Konnyu et al., 2023a).
- Age alone is not the determining factor — the key consideration is whether knee disease is significantly limiting your function and quality of life (Konnyu et al., 2023a).
- If you have another health condition affecting your movement or thinking, let your rehabilitation team know — OT and PT have specific strategies to support complex recoveries (Kim et al., 2026).
For Clinicians
- Osteoarthritis is the primary indication for TKA, but patients with neurological comorbidities (stroke, PD, MS) require integrated rehabilitation plans that address both knee recovery and the underlying condition (Konnyu et al., 2023a; Kim et al., 2026).
- Pre-surgical conservative management through PT and OT should be optimized before TKA referral; functional outcomes are better when patients enter surgery with stronger baseline muscle function (Konnyu et al., 2023b).
- Refer patients with complex ADL, home environment, or cognitive concerns to OT pre-surgically — early identification of barriers to safe discharge reduces hospital length of stay (Kim et al., 2026).
3. Types of Knee Replacement Surgery
Understanding the type of knee replacement helps patients, families, and rehabilitation providers plan the appropriate rehabilitation approach and precautions. The most common procedure is total knee arthroplasty (TKA), in which both the femoral (thigh bone) and tibial (shin bone) joint surfaces are replaced, along with the undersurface of the kneecap in many cases. A partial knee replacement (unicompartmental arthroplasty) replaces only the most damaged compartment of the knee and is appropriate for a smaller subset of patients with disease confined to one part of the joint (Konnyu et al., 2023a).
The vast majority of TKA procedures do not impose strict joint precautions equivalent to posterior hip replacement, but patients are guided through specific early movement restrictions and activity progressions by their surgical and rehabilitation team. Weight-bearing status after TKA is typically full weight-bearing as tolerated from day one, which supports earlier mobilization and functional recovery compared to hip replacement (Konnyu et al., 2023a; Jia et al., 2024).
Rehabilitation protocols vary by surgeon, institution, and individual patient factors. OT and PT must clarify the specific postoperative plan with the surgical team before beginning rehabilitation, as exercise parameters, activity restrictions, and expected milestones differ across programs (Konnyu et al., 2023a).
For Patients and Families
- Unlike hip replacement, knee replacement does not typically involve strict joint precautions — but your surgeon and PT will give you specific activity guidelines for the early recovery period (Konnyu et al., 2023a).
- Most people are allowed to put full weight through the leg from day one after TKA, which helps start recovery quickly (Jia et al., 2024).
- A partial knee replacement has a shorter recovery than a total replacement — your rehabilitation team will adjust the program based on which type you had (Konnyu et al., 2023a).
For Clinicians
- Continuous passive motion (CPM) after TKA does not produce significant improvements in range of motion or patient satisfaction compared to physical therapy alone, and significantly increases length of stay and hospitalization costs — CPM is not routinely recommended (Jia et al., 2024).
- Early weight-bearing as tolerated is standard after TKA and facilitates faster functional recovery; rehabilitation programs should build on this from the first postoperative day (Konnyu et al., 2023a).
- Rehabilitation protocols should be individualized based on surgical approach, implant type, comorbidities, and patient goals (Konnyu et al., 2023a).
4. Prehabilitation: Getting Ready for Surgery
Prehabilitation refers to rehabilitation interventions — exercise, education, or both — initiated before knee replacement surgery with the goal of improving preoperative fitness and optimizing postoperative recovery (Konnyu et al., 2023b). Evidence consistently shows that patients who enter TKA surgery in better physical condition recover faster and with fewer complications than those who do not (Konnyu et al., 2023b).
(Konnyu et al., 2023b). Evidence consistently shows that patients who enter TKA surgery in better physical condition recover faster and with fewer complications than those who do not (Konnyu et al., 2023b).
A systematic review of 13 TKA RCTs found that prehabilitation may improve postoperative strength and reduce length of hospital stay, although heterogeneity across programs limits definitive conclusions for pain and range of motion outcomes (Konnyu et al., 2023b). A separate overview of systematic reviews confirmed that structured prehabilitation before THA and TKA reduces complication rates and improves objective and subjective postoperative outcomes, with effects generally confined to the first 6 months after surgery (Konnyu et al., 2023b).
Occupational therapy contributes to prehabilitation by assessing the home environment before surgery, arranging adaptive equipment, and educating patients on what daily activities will look like during recovery. Physical therapy contributes targeted strengthening of the quadriceps, hamstrings, and hip muscles that drive postoperative functional recovery. Even a 4 to 6 week structured prehabilitation program before elective TKA produces clinically meaningful benefits (Konnyu et al., 2023b).
For Patients and Families
- Doing exercise before your surgery — even for 4 to 6 weeks — helps you recover faster and with fewer complications afterward (Konnyu et al., 2023b).
- Prehabilitation is not just for young or fit patients — it benefits people across all fitness levels, especially those who have been less active due to knee pain (Konnyu et al., 2023b).
- Ask your surgical team for a prehabilitation referral when your surgery is scheduled — starting before you need it is the whole point (Konnyu et al., 2023b).
For Clinicians
- A systematic review of 13 TKA RCTs found prehabilitation may improve postoperative strength and reduce length of stay, with low-strength evidence for equivalence in pain, range of motion, and ADLs (Konnyu et al., 2023b).
- An overview of systematic reviews confirmed prehabilitation reduces complication rates and improves objective and subjective outcomes after TKA, with effects strongest in the first 6 months postoperatively (Konnyu et al., 2023b).
- Pre-surgical OT assessment for home preparation and adaptive equipment provision reduces post-discharge complications and improves patient confidence — this should be standard for all elective TKA patients (Kim et al., 2026).
5. Who Provides Knee Replacement Rehabilitation?
Knee replacement rehabilitation is delivered by a multidisciplinary team whose roles overlap and complement each other across the surgical episode of care (Konnyu et al., 2023a; Kim et al., 2026):
- Occupational therapy (OT): ADL training, adaptive equipment, home safety assessment, return to meaningful activities, and functional discharge planning (Kim et al., 2026).
- Physical therapy (PT): Exercise prescription, strengthening, gait training, range of motion, manual therapy, balance, fall prevention, and functional mobility (Konnyu et al., 2023a; Lim & Kim, 2025).
- Speech-language pathology (SLP): Cognitive-communication support for patients whose memory, attention, or communication difficulties affect their ability to follow rehabilitation instructions or adhere to home exercise programs.
- Orthopaedic surgeon: Surgical decision-making, implant selection, postoperative medical management, and long-term follow-up.
- Nursing: Immediate postoperative wound care, pain management, medication administration, and early mobility support.
- Social work: Discharge planning, home care coordination, equipment funding, and community support services.
For Patients and Families
- You will likely work with both an OT and a PT after knee replacement — they have different but complementary roles, and both are important to a full recovery (Konnyu et al., 2023a; Kim et al., 2026).
- If you have trouble remembering instructions, following multi-step directions, or communicating with your care team, let them know — an SLP can help bridge that gap and support your rehabilitation participation.
- Social work can help arrange home care, equipment funding, and transport for follow-up appointments — do not hesitate to ask about these services before discharge.
For Clinicians
- OT involvement in TKA rehabilitation is supported by systematic review evidence for reducing hospital length of stay and supporting functional ADL outcomes — OT should be integrated into TKA care pathways as a standard component, not an optional add-on (Kim et al., 2026).
- SLP referral is indicated when cognitive-communication barriers (attention, memory, executive function, language) limit a patient’s ability to learn, follow, and self-manage a home exercise program — this is especially relevant for older adults or those with neurological comorbidities.
- A systematic review of 53 RCTs confirmed that diverse TKA rehabilitation programs do not differ significantly in harm outcomes, supporting flexible, patient-centered program design (Konnyu et al., 2023a).
6. Occupational Therapy After Knee Replacement
Occupational therapy after knee replacement focuses on ensuring that patients can safely perform their daily activities while the knee heals, and on supporting a full return to meaningful occupations — work, caregiving, recreation, and community participation — as recovery progresses (Kim et al., 2026). A systematic review of international evidence on OT interventions for TKR found relatively strong evidence that OT contributes to reductions in hospital length of stay, with OT-inclusive rehabilitation pathways supporting safer and more timely discharge (Kim et al., 2026).
Key OT interventions after knee replacement include activities of daily living (ADL) training, adaptive equipment prescription, home assessment and modification, energy conservation, transfer training, and return-to-work or return-to-driving planning (Kim et al., 2026). OTs address practical barriers that PT cannot address alone — including bathroom safety, kitchen access, getting in and out of a car, managing stairs, and returning to caregiving roles (Kim et al., 2026). See the ADLs and Bathing and Shower Safety pages for related guidance.
training, adaptive equipment prescription, home assessment and modification, energy conservation, transfer training, and return-to-work or return-to-driving planning (Kim et al., 2026). OTs address practical barriers that PT cannot address alone — including bathroom safety, kitchen access, getting in and out of a car, managing stairs, and returning to caregiving roles (Kim et al., 2026). See the ADLs and Bathing and Shower Safety pages for related guidance.
For patients with pre-existing conditions such as traumatic brain injury, dementia, or cognitive impairment, OT also addresses the cognitive demands of managing a home exercise program, pain medication schedules, and wound care safely and independently (Kim et al., 2026).
For Patients and Families
- An OT will help you figure out how to dress, shower, use the toilet, cook, and get around your home safely while your knee is healing (Kim et al., 2026).
- OT can recommend and train you on adaptive equipment — such as a raised toilet seat, shower chair, reacher, and long-handled tools — that make daily activities manageable and safe during recovery (Kim et al., 2026).
- If possible, have your OT assess your home before surgery. Getting equipment in place and hazards removed before you return home makes the first days of recovery significantly safer (Kim et al., 2026).
For Clinicians
- A systematic review of international evidence found OT contributes to reduced hospital length of stay after TKR, with OT-inclusive rehabilitation pathways supporting safer discharge (Kim et al., 2026).
- OT pre-surgical home assessment and adaptive equipment education reduces post-discharge complications and improves patient confidence — particularly important given the trend toward same-day and short-stay TKA (Kim et al., 2026).
- OT referral should be standard for all TKA patients, not reserved for those with identified deficits. Proactive OT involvement before and after surgery improves functional discharge outcomes (Kim et al., 2026).
7. Physical Therapy After Knee Replacement
Physical therapy is the cornerstone of TKA rehabilitation, addressing the significant muscle weakness, range of motion deficits, gait dysfunction, and pain that persist after surgery. A systematic review of 53 RCTs confirmed that structured rehabilitation programs produce meaningful improvements in pain, range of motion, and activities of daily living after total knee arthroplasty (Konnyu et al., 2023a). PT begins on the day of or day after surgery and continues across inpatient, home, and outpatient settings.
in pain, range of motion, and activities of daily living after total knee arthroplasty (Konnyu et al., 2023a). PT begins on the day of or day after surgery and continues across inpatient, home, and outpatient settings.
Resistance training is a central component of TKA rehabilitation. A systematic review and meta-analysis found that resistance training significantly improves pain (SMD: 0.84), muscle strength (SMD: 1.03), self-reported function (SMD: 1.58), and performance-based function (SMD: 0.74) in TKA patients, with particularly strong effects when implemented as a standalone intervention or for durations under 12 weeks (Lim & Kim, 2025). Lower-limb active resistance exercise also significantly improves walking speed, Timed Up and Go performance, knee flexion and extension power, and pain intensity compared to conventional rehabilitation (Wei et al., 2024).
Manual therapy after TKA addresses postoperative pain and joint stiffness through mobilization and soft tissue techniques, and is a useful component of a multimodal rehabilitation program alongside exercise (Sahni et al., 2025). For patients at elevated fall risk, PT integrates fall prevention strategies including balance training, walking aid progression, and stair training. For patients with back pain, osteoarthritis in other joints, or prior hip replacement, PT must account for these comorbidities when designing the program.
For Patients and Families
- Resistance exercises are the most effective rehabilitation strategy after knee replacement for improving pain, strength, and function — your PT will design a progressive program tailored to your recovery stage (Lim & Kim, 2025).
- Your home exercise program is where most of your recovery happens — doing your exercises daily is more important than any single clinic visit (Konnyu et al., 2023a).
- Manual therapy from your PT — hands-on joint mobilization and soft tissue work — can significantly reduce knee pain and stiffness in the weeks after surgery (Sahni et al., 2025).
For Clinicians
- Resistance training significantly improves pain (SMD: 0.84), muscle strength (SMD: 1.03), self-reported function (SMD: 1.58), and performance-based function (SMD: 0.74) in TKA patients — resistance training should be the primary modality in post-TKA PT programs (Lim & Kim, 2025).
- Lower-limb active resistance exercise significantly improves walking speed and TUG performance compared to conventional rehabilitation in TKA patients across 14 RCTs with approximately 880 participants (Wei et al., 2024).
- Manual therapy is a useful adjunct to exercise in post-TKA rehabilitation for pain management; a multimodal PT program combining exercise and manual therapy is preferable to either alone (Sahni et al., 2025).
8. Telerehabilitation After Knee Replacement
Telerehabilitation — rehabilitation delivered via videoconference, digital platforms, or remote monitoring — is an evidence-supported alternative to in-person rehabilitation after knee replacement, with important implications for access, compliance, and cost (Tsang et al., 2024). Geographic barriers, transportation limitations, early postoperative mobility restrictions, and the shift toward shorter hospital stays have all increased demand for remote rehabilitation options after TKA.
A systematic review and meta-analysis of 11 RCTs involving 1,825 patients confirmed that telerehabilitation produces comparable improvements in pain and functional outcomes to conventional in-person rehabilitation after total knee replacement, with no significant difference in standardized mean difference for pain or physical function (Tsang et al., 2024). Telerehabilitation also significantly reduces hospital resource utilization and costs compared to in-person rehabilitation (Tsang et al., 2024). A separate systematic review confirmed equivalent outcomes between outpatient and home-based rehabilitation programs after knee arthroplasty across range of motion, knee scores, and functional outcomes (Zhao et al., 2023).
Occupational therapy via telehealth can support home exercise program coaching, adaptive equipment guidance, and functional activity problem-solving for patients who cannot attend in person. Physical therapy via telehealth can deliver exercise instruction, movement analysis, and progressive program updates. For patients with limited technological literacy — especially older adults — OT support with device setup and digital navigation may be needed before telerehabilitation begins (Tsang et al., 2024).
For Patients and Families
- Research confirms that telerehabilitation after knee replacement produces equivalent outcomes to in-person rehabilitation — if getting to a clinic is difficult, remote therapy is a real and effective option (Tsang et al., 2024).
- Telerehabilitation significantly reduces travel burden and healthcare costs without compromising your recovery (Tsang et al., 2024).
- Whether you do outpatient or home-based rehabilitation, outcomes are similar — what matters most is consistency and following your home exercise program (Zhao et al., 2023).
For Clinicians
- A meta-analysis of 11 RCTs (1,825 patients) found telerehabilitation produces equivalent pain and functional outcomes to in-person rehabilitation after TKR, with significantly lower hospital resource utilization (Tsang et al., 2024).
- Outpatient and home-based rehabilitation produce no clinically significant differences in ROM, knee scores, or functional outcomes after knee arthroplasty — rehabilitation setting should be determined by patient access, preference, and support (Zhao et al., 2023).
- Telerehabilitation is most appropriate for follow-up sessions and home program progression; initial assessment and early postoperative management benefit from in-person contact, particularly for gait training and manual therapy (Konnyu et al., 2023a).
9. What to Expect During Recovery
Knee replacement recovery follows a broadly predictable timeline, though individual variation is significant based on age, preoperative function, fitness, comorbidities, and engagement with rehabilitation (Konnyu et al., 2023a). Active participation in rehabilitation is the single strongest modifiable predictor of outcome.
 Hospital Stay (typically 1–2 days)
Hospital Stay (typically 1–2 days)
- PT begins walking with a walking aid on the day of or day after surgery — early mobilization reduces complications (Konnyu et al., 2023a).
- OT provides ADL training, adaptive equipment instruction, and discharge planning before you leave hospital (Kim et al., 2026).
- Pain is managed with a multimodal approach including nerve blocks, anti-inflammatories, and as-needed opioids.
- Discharge home or to a short-term rehabilitation facility is determined by support, home environment, and functional status (Konnyu et al., 2023a).
First 6 Weeks
- Swelling, bruising, and pain gradually reduce — icing and elevation help manage this (Konnyu et al., 2023a).
- PT focuses on range of motion, quadriceps activation, walking progression, and stair training (Lim & Kim, 2025).
- OT supports safe performance of dressing, bathing, and household tasks with a healing knee (Kim et al., 2026).
- Home exercise compliance during this period is a key predictor of 3-month outcomes (Konnyu et al., 2023a).
6 Weeks to 3 Months
- PT progresses to more demanding resistance training, functional exercise, and community mobility (Lim & Kim, 2025; Wei et al., 2024).
- Most people return to driving, light work, and community activities during this period (Konnyu et al., 2023a).
- Residual stiffness or swelling should be discussed with the surgical team and PT (Jia et al., 2024).
3 to 12 Months
- Continued strength and functional gains — full recovery typically takes 6 to 12 months (Konnyu et al., 2023a).
- Adapted physical activity programs designed for post-TKA patients improve quality of life and function when continued 6 months after surgery (Zinno et al., 2025).
- Return to recreational activities and sport for appropriate patients with PT guidance (Konnyu et al., 2023a).
 When to Request OT, PT, or SLP Referral
When to Request OT, PT, or SLP Referral
Refer to Occupational Therapy (OT) when:
- Surgery is scheduled — pre-surgical OT home assessment and adaptive equipment preparation improves discharge safety (Kim et al., 2026).
- The patient is being discharged home and daily activity management, safety, or equipment needs have not been addressed (Kim et al., 2026).
- ADL performance — dressing, bathing, toileting, transfers — is limited by the healing knee (Kim et al., 2026).
- Cognitive, behavioural, or complex social factors may affect safe self-management at home after discharge (Kim et al., 2026).
- Return to work, driving, or caregiving roles requires functional assessment and adaptive planning (Kim et al., 2026).
Refer to Physical Therapy (PT) when:
- Surgery is scheduled — prehabilitation PT improves postoperative strength and reduces hospital stay (Konnyu et al., 2023b).
- The patient is mobilizing after TKA — PT begins day of or day after surgery in hospital (Konnyu et al., 2023a).
- Range of motion, strength, gait, balance, or functional mobility are impaired — the standard indication for post-TKA PT (Konnyu et al., 2023a; Lim & Kim, 2025).
- Fall risk is present — PT addresses balance, walking aid progression, and fall prevention (Konnyu et al., 2023a).
- In-person attendance is difficult — telerehabilitation is an evidence-supported equivalent option (Tsang et al., 2024).
Refer to Speech-Language Pathology (SLP) when:
- Cognitive-communication barriers limit the patient’s ability to learn or follow a home exercise program — supporting adherence is a key outcome predictor (Konnyu et al., 2023a).
- The patient has a neurological comorbidity (TBI, stroke, dementia, PD) affecting rehabilitation participation and communication with the care team.
- Dysphagia or swallowing concerns are present in the perioperative period requiring SLP assessment and management.
Also See
- Hip Replacement & Recovery — Complementary page covering prehabilitation, hip precautions, OT, and PT after THA
- Osteoarthritis — Conservative OT and PT management of knee OA before surgery becomes necessary
- Fall Prevention — Balance assessment and exercise programs for patients with elevated fall risk after TKA
- Activities of Daily Living (ADLs) — Adaptive strategies and equipment for daily independence during recovery
- Bathing and Shower Safety — Adaptive equipment and OT strategies for safe bathing during recovery
- Back Pain — Often co-occurring with knee OA; OT and PT management overlap significantly
- Home Modification and Safety — Room-by-room safety assessment and modifications to support recovery at home
References
Jia, Z., Zhang, Y., Zhang, W., Xu, C., & Liu, W. (2024). Efficacy and safety of continuous passive motion and physical therapy in recovery from knee arthroplasty: A systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research, 19, 68. https://doi.org/10.1186/s13018-024-04536-y
Kim, J. A., Ha, S.-K., & Jung, M.-Y. (2026). A systematic review of international evidence to inform occupational therapy practice guidelines for total knee replacement in the Korean health system. Occupational Therapy International, 2026, 5583913. https://doi.org/10.1155/oti/5583913
Konnyu, K. J., Thoma, L. M., Cao, W., Aaron, R. K., Panagiotou, O. A., Bhuma, M. R., Adam, G. P., Balk, E. M., & Pinto, D. (2023a). Rehabilitation for total knee arthroplasty: A systematic review. American Journal of Physical Medicine & Rehabilitation, 102(1), 19–33. https://doi.org/10.1097/PHM.0000000000002008
Konnyu, K. J., Thoma, L. M., Cao, W., Aaron, R. K., Panagiotou, O. A., Bhuma, M. R., Adam, G. P., Pinto, D., & Balk, E. M. (2023b). Prehabilitation for total knee or total hip arthroplasty: A systematic review. American Journal of Physical Medicine & Rehabilitation, 102(1), 1–10. https://doi.org/10.1097/PHM.0000000000002006
Lim, J., & Kim, B. (2025). Effects of resistance training on pain, muscle strength, and function in patients undergoing total knee arthroplasty: A systematic review and meta-analysis. Journal of Clinical Medicine, 14(14), 4979. https://doi.org/10.3390/jcm14144979
Sahni, S., Fares, J. E., & Jordan, H. (2025). Manual therapy in post-operative knee management: A systematic review of effects on pain in total knee replacement (TKR) patients. Cureus, 17(9), e92734. https://doi.org/10.7759/cureus.92734
Tsang, M. P., Man, G. C. W., Xin, H., Chong, Y. C., Ong, M. T.-Y., & Yung, P. S.-H. (2024). The effectiveness of telerehabilitation in patients after total knee replacement: A systematic review and meta-analysis of randomized controlled trials. Journal of Telemedicine and Telecare, 30(5), 795–808. https://doi.org/10.1177/1357633X221097469
Wei, G., Shang, Z., Li, Y., Wu, Y., & Zhang, L. (2024). Effects of lower-limb active resistance exercise on mobility, physical function, knee strength and pain intensity in patients with total knee arthroplasty: A systematic review and meta-analysis. BMC Musculoskeletal Disorders, 25, 730. https://doi.org/10.1186/s12891-024-07845-9
Zhao, B., Liu, H., Du, K., Zhou, W., & Li, Y. (2023). Effectiveness and safety of outpatient rehabilitation versus home-based rehabilitation after knee arthroplasty: A systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research, 18, 704. https://doi.org/10.1186/s13018-023-04160-2
Zinno, R., Pinelli, E., Barone, G., Dallari, D., Scoppolini Massini, M., & Bragonzoni, L. (2025). Effectiveness of adapted physical activity on quality of life of patients with knee and hip replacement: A randomized pilot study. Healthcare, 13(18), 2333. https://doi.org/10.3390/healthcare13182333
© TherapyTopics.com — All information is for educational purposes only and does not constitute medical or therapeutic advice. Consult a licensed therapist or physician for evaluation and treatment.