

Key Takeaways
- Shoulder pain affects 7 to 26% of the general population and is one of the most common musculoskeletal conditions seen across rehabilitation settings (Lucas et al., 2022).
- Exercise therapy is the recommended first-line treatment for rotator cuff related shoulder pain, with strong evidence supporting active, progressive strengthening programs (Desmeules et al., 2025).
- Occupational therapy addresses how shoulder pain limits daily activities, work, self-care, and meaningful participation, including ergonomic assessment and return-to-work planning (Lafrance et al., 2022).
- Manual therapy combined with exercise does not consistently outperform exercise alone for rotator cuff related shoulder pain; exercise is the primary modality (Paraskevopoulos et al., 2023).
- Telerehabilitation for shoulder conditions produces equivalent pain and range of motion outcomes to in-person rehabilitation, with particular benefits for longer program durations (Lin et al., 2025).
- Early rehabilitation after rotator cuff repair accelerates range of motion recovery without increasing re-tear rates (Chen et al., 2024).
Contents
- What Is Rotator Cuff Related Shoulder Pain?
- Who Is Affected?
- Types of Shoulder Conditions
- Occupational Therapy’s Role
- Physical Therapy’s Role
- Speech-Language Pathology’s Role
- Exercise Therapy
- Manual Therapy
- Post-Surgical Rehabilitation
- Work-Related Shoulder Pain
- Telerehabilitation for Shoulder Conditions
- When to Refer
- References
1. What Is Rotator Cuff Related Shoulder Pain?
Rotator cuff related shoulder pain (RCRSP) is the term now recommended by international clinical practice guidelines to describe the most common category of shoulder pain seen in rehabilitation settings (Desmeules et al., 2025). It encompasses conditions previously labeled subacromial impingement syndrome, subacromial pain syndrome, rotator cuff tendinopathy, subacromial bursitis, and calcific tendinopathy. The shift to RCRSP reflects a growing understanding that specific structural diagnoses based on clinical examination alone are unreliable, and that treatment should target functional impairments rather than assumed structural causes (Desmeules et al., 2025).
The rotator cuff is a group of four muscles and their tendons that surround and stabilize the shoulder joint. These muscles control rotation and elevation of the arm and are essential for nearly all overhead and reaching activities. Rotator cuff related pain typically develops gradually and is associated with shoulder weakness, pain with overhead movements, and limited range of motion. In some cases, a partial or full thickness rotator cuff tear is present, which may require surgical repair in selected patients (Desmeules et al., 2025).
The biopsychosocial model is now the recommended framework for understanding RCRSP. Biological factors including age-related tendon changes and muscle strength deficits, psychological factors including fear of movement and pain catastrophizing, and social factors including work demands and access to care all contribute to onset, severity, and recovery (Desmeules et al., 2025).
🟢 For Patients and Families
- Rotator cuff related shoulder pain is the most common cause of shoulder pain and is highly treatable with rehabilitation (Desmeules et al., 2025).
- You do not need a specific structural diagnosis to begin effective rehabilitation. Exercise and education are the first-line treatments regardless of imaging findings (Desmeules et al., 2025).
- Many people with shoulder pain on imaging have no symptoms, and many with significant pain have normal imaging. What matters most for treatment is your function and goals, not the image (Desmeules et al., 2025).
🟣 For Clinicians
- The 2025 JOSPT clinical practice guideline recommends moving away from structural diagnostic labels toward RCRSP as an umbrella term, and prioritizing active rehabilitation over passive treatments (Desmeules et al., 2025).
- Subacromial decompression surgery is not recommended for rotator cuff tendinopathy in the absence of full-thickness rotator cuff tears (Desmeules et al., 2025).
- Psychosocial screening for pain catastrophizing, kinesiophobia, and depression is recommended as part of initial shoulder pain assessment (Desmeules et al., 2025).
2. Who Is Affected?
Shoulder pain affects 7 to 26% of the general population, making it one of the most prevalent musculoskeletal conditions worldwide. Incidence ranges from 7.7 to 62 per 1,000 persons per year depending on the population studied (Lucas et al., 2022). Shoulder pain is particularly prevalent in working-age adults and in occupations involving repetitive arm use, overhead work, and forceful exertions.
Work-related physical exposures are strongly associated with the development of rotator cuff disorders. Shoulder elevation, repetition, forceful exertions, and whole-body vibration have the strongest evidence for increasing the risk of shoulder tendinopathy and impingement in working populations (Versloot et al., 2024). Occupations in manufacturing, construction, healthcare, and agriculture carry the highest shoulder disorder burden.
and whole-body vibration have the strongest evidence for increasing the risk of shoulder tendinopathy and impingement in working populations (Versloot et al., 2024). Occupations in manufacturing, construction, healthcare, and agriculture carry the highest shoulder disorder burden.
People with neurological conditions such as stroke, multiple sclerosis, or Parkinson’s disease also experience high rates of shoulder pain due to altered muscle tone, reduced movement, and compensatory posture. For patients with traumatic brain injury or cerebral palsy, shoulder pain management requires integration with the primary neurological rehabilitation plan (Desmeules et al., 2025).
🟢 For Patients and Families
- Shoulder pain is extremely common, affecting up to 1 in 4 adults at some point in their lives, so you are not alone and effective treatment is available (Lucas et al., 2022).
- If your job involves repetitive overhead work or forceful arm use, your work environment may be contributing to your shoulder pain. Your OT and PT can help identify modifications to reduce ongoing strain (Versloot et al., 2024).
- If you have a neurological condition alongside shoulder pain, your rehabilitation team needs to address both together rather than separately for the best outcome (Desmeules et al., 2025).
🟣 For Clinicians
- Global shoulder pain prevalence ranges from 7 to 26% with incidence of 7.7 to 62 per 1,000 persons per year; shoulder disorders account for a substantial proportion of all musculoskeletal healthcare utilization (Lucas et al., 2022).
- Physical work exposures including shoulder elevation, repetition, force, and vibration have the strongest evidence for association with rotator cuff disorders in occupational populations (Versloot et al., 2024).
- Screen for co-occurring neurological conditions and integrate shoulder rehabilitation with primary neurological management for patients with stroke, TBI, MS, or CP (Desmeules et al., 2025).
3. Types of Shoulder Conditions
The most common shoulder conditions seen in rehabilitation settings fall under the RCRSP umbrella. Rotator cuff tendinopathy refers to degeneration or irritation of the rotator cuff tendons, typically presenting with pain during overhead activities and shoulder weakness. Subacromial bursitis involves inflammation of the bursa between the rotator cuff and the acromion bone. Calcific tendinopathy involves calcium deposits within the rotator cuff tendons and can cause intense acute pain. Partial and full thickness rotator cuff tears range from minor fraying to complete disruption of one or more tendons (Desmeules et al., 2025).
Other common shoulder conditions include adhesive capsulitis (frozen shoulder), characterized by progressive pain and severe restriction of both active and passive shoulder movement; glenohumeral osteoarthritis; acromioclavicular joint disorders; and shoulder instability. While these conditions have distinct presentations and management approaches, many share core rehabilitation principles including therapeutic exercise, education, and activity modification (Desmeules et al., 2025).
For older adults, degenerative rotator cuff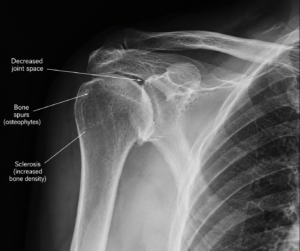 tears are extremely common and are often asymptomatic. The presence of a tear on imaging does not by itself determine whether surgery is required or whether the tear is the source of symptoms. Guidelines strongly recommend conservative rehabilitation before surgical referral for most rotator cuff conditions (Desmeules et al., 2025).
tears are extremely common and are often asymptomatic. The presence of a tear on imaging does not by itself determine whether surgery is required or whether the tear is the source of symptoms. Guidelines strongly recommend conservative rehabilitation before surgical referral for most rotator cuff conditions (Desmeules et al., 2025).
🟢 For Patients and Families
- A rotator cuff tear on an MRI does not automatically mean you need surgery. Many people with rotator cuff tears respond very well to physical therapy and occupational therapy (Desmeules et al., 2025).
- Frozen shoulder (adhesive capsulitis) is a separate condition from rotator cuff pain and follows a different rehabilitation timeline. Your therapist will adjust your program based on your specific diagnosis (Desmeules et al., 2025).
- Surgery is typically considered only after a structured rehabilitation program has been completed without adequate improvement (Desmeules et al., 2025).
🟣 For Clinicians
- Conservative rehabilitation is recommended as first-line management for rotator cuff tendinopathy, partial thickness tears, and most full thickness tears before surgical referral (Desmeules et al., 2025).
- Subacromial decompression surgery is not recommended for rotator cuff tendinopathy without full-thickness tears; evidence does not support it outperforming sham surgery (Desmeules et al., 2025).
- Differentiate RCRSP from adhesive capsulitis, glenohumeral OA, and cervical radiculopathy early in assessment, as these conditions require distinct management pathways (Desmeules et al., 2025).
4. Occupational Therapy’s Role
Occupational therapists bring a function-centered perspective to shoulder pain rehabilitation that complements PT-led exercise. OT examines how shoulder pain and weakness limit a person’s ability to perform daily activities, including dressing, grooming, cooking, driving, childcare, recreational activities, and work tasks. When the shoulder is painful or weak, people compensate in ways that can lead to further injury, fatigue, and reduced independence (Lafrance et al., 2022).
Core OT interventions for shoulder pain include activities of daily living assessment and training, adaptive equipment prescription (such as reachers, dressing aids, and ergonomic tools), home environment modification, energy conservation, and pain management strategies during daily tasks. Ergonomic workstation assessment is a central OT contribution for patients whose shoulder pain is work-related, addressing posture, tool use, task rotation, and workplace design to reduce ongoing rotator cuff loading (Lafrance et al., 2022).
Return-to-work planning is explicitly included in the 2022 JOSPT clinical practice guideline for rotator cuff disorders, which recommends that a return-to-work plan be developed early in collaboration with the worker and other stakeholders, combining multiple strategies to promote successful return (Lafrance et al., 2022). OT is the lead discipline for functional capacity assessment, job demands analysis, and graduated return-to-work planning in these cases. For patients with neurological conditions involving shoulder pain, OT also addresses home modification, positioning, and adaptive strategies relevant to the underlying neurological impairment.
🟢 For Patients and Families
- An OT can help you find ways to manage dressing, cooking, driving, and other daily activities while protecting your shoulder during recovery (Lafrance et al., 2022).
- If your shoulder pain is related to your job, OT can assess your workstation and tasks and recommend specific changes to reduce the load on your rotator cuff (Lafrance et al., 2022).
- A return-to-work plan developed early in your recovery produces better outcomes than waiting until pain is fully resolved before addressing work goals (Lafrance et al., 2022).
🟣 For Clinicians
- The 2022 JOSPT clinical practice guideline for rotator cuff disorders explicitly recommends early return-to-work planning involving a multidisciplinary team, with OT playing a central role in functional capacity evaluation and job demands analysis (Lafrance et al., 2022).
- OT ergonomic assessment and worksite modification are evidence-supported components of shoulder disorder rehabilitation in occupational populations (Versloot et al., 2024).
- OT referral is indicated when shoulder pain is limiting ADL performance, work tasks, self-care, or meaningful participation beyond what exercise alone addresses (Lafrance et al., 2022).
5. Physical Therapy’s Role
Physical therapy is the cornerstone of non-surgical shoulder pain management. PT assessment for RCRSP includes evaluation of shoulder range of motion, strength, scapular control, posture, movement patterns, and functional activities. This comprehensive evaluation informs an individualized rehabilitation program that targets the specific impairments contributing to each patient’s pain and limitation (Desmeules et al., 2025).
The 2025 clinical practice guideline strongly recommends prescribing an active, task-oriented rehabilitation program combining exercise and education to reduce pain and disability in adults with rotator cuff disorders (Desmeules et al., 2025). Specific exercise, manual therapy (where appropriate), and pain neuroscience education are the primary PT tools. PT also addresses strength deficits, which are consistently present in RCRSP. A systematic review confirmed that rehabilitation interventions improve shoulder strength, with active exercise and strength training producing the strongest effects for rotator cuff related weakness (Zhang et al., 2026).
For patients with shoulder pain alongside back pain, osteoarthritis, post-surgical recovery, or fall risk, PT integrates shoulder rehabilitation with management of the broader musculoskeletal presentation. Exercise programs are progressive, tailored to the patient’s presentation, and designed to build toward return to the specific functional demands of the patient’s daily life and work (Lafrance et al., 2024).
🟢 For Patients and Families
- Physical therapy for shoulder pain focuses on progressive exercises that gradually rebuild strength and movement, not just on temporary pain relief (Desmeules et al., 2025).
- Building strength in the rotator cuff and surrounding shoulder muscles is one of the most important parts of recovery. Your PT will design a progressive program specific to your needs (Zhang et al., 2026).
- Consistent participation in your home exercise program is the most important factor in recovery, more than any individual clinic treatment session (Lafrance et al., 2024).
🟣 For Clinicians
- The 2025 CPG strongly recommends active, task-oriented programs combining exercise and education as first-line management for rotator cuff disorders (Desmeules et al., 2025).
- Active exercise and strength training improve shoulder strength across multiple intervention types, with eccentric exercise producing the largest effect (SMD 0.85) and motor control exercise also demonstrating benefit (Zhang et al., 2026).
- Exercise prescription for RCRSP should specify type, intensity, progression, and frequency rather than providing generic rotator cuff exercise programs without structure (Lafrance et al., 2024).
6. Speech-Language Pathology’s Role
Speech-language pathologists (SLPs) contribute to shoulder pain rehabilitation in several clinical contexts. In patients with neurological conditions including stroke, TBI, or dementia where shoulder pain co-occurs with cognitive or communication impairments, SLP ensures that rehabilitation instructions, home exercise programs, and self-management strategies are delivered in accessible formats that the patient can reliably follow.
For patients with dysphagia who have undergone cervical or shoulder surgery, SLP assessment and management of swallowing function is indicated where relevant. In complex pain presentations with significant cognitive-communication barriers, SLP supports the interprofessional team by bridging communication between patient and providers, adapting health literacy materials, and facilitating consistent self-management of exercise programs where adherence is a concern (Desmeules et al., 2025).
In pediatric populations where shoulder pain occurs in the context of conditions such as cerebral palsy, SLP collaborates with OT and PT to ensure that communication supports and sensory-motor considerations are integrated into the rehabilitation plan.
🟢 For Patients and Families
- If a neurological condition makes it difficult to understand or follow your shoulder rehabilitation program, an SLP can help adapt instructions and support consistent participation.
- For patients who have had neck or shoulder surgery and experience swallowing difficulties, an SLP can assess and treat swallowing function as part of the recovery team.
- Children with conditions affecting communication who also have shoulder pain can benefit from SLP involvement to ensure therapy is accessible and goals are clearly communicated.
🟣 For Clinicians
- SLP referral is indicated when cognitive-communication barriers limit a patient’s ability to engage with, retain, or self-manage a shoulder rehabilitation program, particularly in neurological populations.
- In patients with cervical pathology alongside shoulder pain, SLP assessment for dysphagia is indicated when swallowing symptoms are present perioperatively or following cervical procedures.
- For pediatric shoulder pain in the context of CP or other neurodevelopmental conditions, SLP-OT-PT collaboration ensures rehabilitation is accessible and goals are consistently communicated across environments.
7. Exercise Therapy
Exercise is the most evidence-supported treatment for rotator cuff related shoulder pain and is recommended as first-line management in all major clinical practice guidelines (Desmeules et al., 2025). The 2024 JOSPT systematic review of 31 RCTs evaluated exercise according to the FITT principle (frequency, intensity, type, and time) and found that specific exercises targeting rotator cuff and scapular muscles produce superior outcomes to non-specific general exercise for reducing shoulder pain and disability (Lafrance et al., 2024).
Strengthening exercises, progressive resistance training, and motor control exercise are the core modalities for RCRSP rehabilitation. Eccentric and concentric loading, neuromuscular control exercises, and scapular stabilization programs all have evidence supporting their use in rotator cuff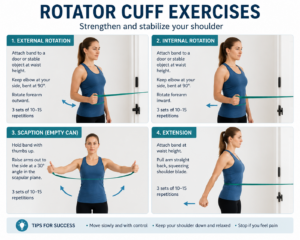 tendinopathy. Rehabilitation interventions that incorporate active exercises or strength training are specifically recommended to address the consistent strength deficits found in people with RCRSP (Zhang et al., 2026).
tendinopathy. Rehabilitation interventions that incorporate active exercises or strength training are specifically recommended to address the consistent strength deficits found in people with RCRSP (Zhang et al., 2026).
Exercise programs should be progressive, individually tailored, and supervised to ensure correct technique and appropriate loading. Poorly prescribed or unsupervised programs are less effective. The FITT principle provides a useful framework for exercise prescription: type should emphasize rotator cuff and scapular specific strengthening, intensity should be sufficient to challenge tissues, frequency of 2 to 3 sessions per week is supported by evidence, and duration of at least 6 to 8 weeks is needed for meaningful gains (Lafrance et al., 2024).
🟢 For Patients and Families
- Specific targeted exercises for the rotator cuff and shoulder blade muscles are more effective than general exercise for shoulder pain. Your PT will design a program aimed at your particular weaknesses (Lafrance et al., 2024).
- Some discomfort during exercise is normal and does not mean you are causing harm. Your PT will guide you on what level of exercise discomfort is acceptable during recovery (Desmeules et al., 2025).
- You need at least 6 to 8 weeks of consistent exercise to see meaningful improvement. Stopping early is one of the most common reasons people do not fully recover (Lafrance et al., 2024).
🟣 For Clinicians
- Specific rotator cuff and scapular exercise outperforms non-specific exercise for shoulder pain and disability in RCRSP across 31 RCTs (Lafrance et al., 2024).
- Active exercises and strength training produce the strongest strength gains in RCRSP, with eccentric loading (SMD 0.85), concentric training (SMD 0.65), and motor control exercise (SMD 0.45) all demonstrating benefit (Zhang et al., 2026).
- Exercise prescription should include specific type, intensity, progression criteria, and frequency to optimize loading rather than relying on generic program templates (Lafrance et al., 2024).
8. Manual Therapy
Manual therapy for shoulder pain includes joint mobilization, manipulation, soft tissue techniques, and trigger point therapy. It is commonly used in combination with exercise in clinical practice. A systematic review and meta-analysis of 12 RCTs found that adding manual therapy to an exercise program does not produce significantly better outcomes for pain during movement (SMD 0.15) or function compared to exercise alone for rotator cuff related shoulder pain (Paraskevopoulos et al., 2023). However, manual therapy may reduce pain at rest and may be valuable for specific presentations where joint stiffness or mobility restriction is a primary contributor.
The 2025 clinical practice guideline for rotator cuff tendinopathy does not recommend manual therapy as a standalone treatment but supports its use as a component of multimodal rehabilitation in selected patients (Desmeules et al., 2025). The most appropriate role of manual therapy is as an adjunct to exercise, particularly in the early stages of rehabilitation when pain is limiting participation in exercise, or when joint stiffness is restricting range of motion.
For patients who have had shoulder surgery, manual therapy during the post-operative period must be guided by surgical precautions and the treating surgeon’s protocol. Gentle range of motion techniques are typically incorporated early in rehabilitation, while more vigorous mobilization is introduced progressively as healing allows (Chen et al., 2024).
🟢 For Patients and Families
- Hands-on therapy from your PT can help reduce pain and improve movement, especially in the early stages of rehabilitation when pain is limiting your ability to exercise (Paraskevopoulos et al., 2023).
- Manual therapy works best as a complement to your exercise program, not as a replacement for it. The exercise you do between sessions drives most of your long-term recovery (Desmeules et al., 2025).
- After shoulder surgery, your PT will follow your surgeon’s guidelines carefully before progressing any hands-on techniques (Chen et al., 2024).
🟣 For Clinicians
- Adding manual therapy to exercise does not significantly improve pain during movement (SMD 0.15) or function compared to exercise alone for RCRSP across 11 RCTs (Paraskevopoulos et al., 2023).
- Manual therapy is most appropriate as an adjunct to exercise in patients with joint stiffness, mobility restrictions, or pain limiting exercise participation, rather than as routine addition for all RCRSP presentations (Desmeules et al., 2025).
- Standalone manual therapy without exercise is not supported by evidence for sustained outcomes in RCRSP and should not be the primary treatment approach (Desmeules et al., 2025).
9. Post-Surgical Rehabilitation
When rotator cuff tears do not respond to conservative management, or when large tears cause significant functional impairment, surgical repair may be indicated. Post-surgical rehabilitation is essential to restore shoulder function, prevent re-tear, and return patients to their prior level of activity. Rehabilitation after rotator cuff repair typically proceeds through phases: initial protection and early motion, intermediate strengthening, and advanced functional training (Chen et al., 2024).
The timing of rehabilitation after rotator cuff surgery is a clinically important decision. A systematic review and meta-analysis of 9 RCTs involving 830 patients found that early rehabilitation after arthroscopic rotator cuff repair accelerates recovery of shoulder range of motion and forward flexion compared to delayed rehabilitation, without significantly increasing re-tear rates (Chen et al., 2024). Early mobilization is therefore generally favored, though protocols vary based on tear size, repair quality, and surgeon preference.
Occupational therapy in the post-surgical period addresses ADL adaptations, sling management, bathing and dressing with a healing shoulder, and gradual return to home and work activities. Physical therapy leads progressive range of motion, strengthening, and functional movement. For patients with pre-existing conditions such as osteoarthritis or neurological comorbidities, post-surgical rehabilitation must account for these factors when setting progression timelines and activity expectations (Desmeules et al., 2025).
🟢 For Patients and Families
- Starting gentle movement early after rotator cuff surgery helps you regain range of motion faster and does not increase the risk of the repair failing (Chen et al., 2024).
- Your OT will help you manage daily tasks safely while your shoulder is healing, including dressing, bathing, and cooking adaptations to protect the repair.
- Recovery after rotator cuff repair typically takes 4 to 6 months and requires consistent engagement with your rehabilitation program throughout (Chen et al., 2024).
🟣 For Clinicians
- Early rehabilitation after arthroscopic rotator cuff repair accelerates recovery of range of motion and forward flexion without significantly increasing re-tear rates across 9 RCTs with 830 patients (Chen et al., 2024).
- Rehabilitation protocols should be coordinated with the surgical team to account for tear size, repair integrity, and individual patient factors that affect safe loading timelines (Chen et al., 2024).
- OT involvement in the post-surgical period addresses ADL safety, sling management, and return-to-work planning, which are critical for short-stay and ambulatory surgical patients (Lafrance et al., 2022).
10. Work-Related Shoulder Pain
Rotator cuff disorders are among the most common work-related musculoskeletal conditions. Physical work exposures including shoulder elevation, repetitive movements, forceful exertions, and whole-body vibration have the strongest evidence for increasing the risk of shoulder tendinopathy and impingement (Versloot et al., 2024). Psychosocial work factors including low job control, poor social support, and high job demands also contribute to onset and chronicity (Versloot et al., 2024).
Effective management of work-related shoulder pain requires a coordinated approach that addresses both the clinical condition and the occupational exposures driving it. The 2022 clinical practice guideline recommends that return-to-work planning begin early and involve the worker, employer, treating clinicians, and, where applicable, occupational health and compensation systems (Lafrance et al., 2022). Early return to modified work, where possible, produces better outcomes than prolonged absence.
Occupational therapy leads functional capacity evaluation, job demands analysis, ergonomic worksite assessment, and graduated return-to-work planning. Physical therapy addresses the functional impairments that limit work capacity through exercise, education, and manual therapy. Together, OT and PT provide the rehabilitation foundation for successful return to occupational participation (Lafrance et al., 2022; Versloot et al., 2024).
🟢 For Patients and Families
- If your shoulder pain is related to your job, a return-to-work plan developed early in your recovery leads to better outcomes than waiting until you are fully recovered (Lafrance et al., 2022).
- Modified or light duties during recovery are preferable to complete time off work. Your OT and PT can communicate with your employer about safe work modifications (Lafrance et al., 2022).
- Workplace changes, including tool modifications, task rotation, and posture adjustments, can reduce ongoing rotator cuff loading and prevent recurrence (Versloot et al., 2024).
🟣 For Clinicians
- The 2022 JOSPT CPG recommends early return-to-work planning incorporating multiple stakeholders and graduated exposure as a core component of rotator cuff disorder management (Lafrance et al., 2022).
- Physical and psychosocial work exposures both contribute to shoulder disorder risk; ergonomic and psychosocial interventions should be considered alongside clinical rehabilitation (Versloot et al., 2024).
- OT-led job demands analysis and worksite assessment are evidence-supported components of occupational shoulder disorder rehabilitation (Lafrance et al., 2022).
11. Telerehabilitation for Shoulder Conditions
Telerehabilitation for shoulder pain is a growing and evidence-supported care model that addresses access barriers including geographic distance, transportation limitations, and work schedules. A systematic review and meta-analysis of RCTs found that telerehabilitation for non-operatively managed shoulder conditions may reduce pain and improve range of motion compared to in-person rehabilitation, with particularly significant benefits when programs lasted 12 weeks or longer (Lin et al., 2025). Patient satisfaction with telerehabilitation for shoulder conditions is generally favorable across studies.
A separate meta-analysis of 10 RCTs with 497 participants confirmed that telemedicine significantly improves shoulder function measured by the Constant-Murley score and the Quick DASH score, reduces visual analog scale pain, and improves range of motion in rotator cuff disorder patients compared to conventional treatment (Zhang et al., 2024). These findings support telemedicine as a viable component of comprehensive shoulder rehabilitation, particularly for follow-up care, home program delivery, and patients who face access barriers to in-person services.
OT and PT can both leverage telerehabilitation for shoulder pain management. OT via telehealth addresses adaptive equipment guidance, ADL coaching, ergonomic assessment, and home program support. PT via telehealth delivers exercise instruction, movement analysis, and progressive program management. For patients with limited technological literacy, particularly older adults, OT support with device setup may be needed to make telerehabilitation accessible (Lin et al., 2025).
🟢 For Patients and Families
- You may be able to receive effective shoulder rehabilitation through video appointments at home. Research shows telerehabilitation can reduce pain and improve shoulder movement, especially in longer programs (Lin et al., 2025).
- Telehealth shoulder therapy is useful for ongoing follow-up, home program coaching, and people who find attending a clinic regularly difficult (Zhang et al., 2024).
- Ask your therapist whether telerehabilitation is appropriate for your condition, as some situations still benefit from in-person assessment or hands-on treatment.
🟣 For Clinicians
- Telerehabilitation may reduce pain and improve range of motion in non-operatively managed shoulder conditions, with greatest benefits in programs of 12 weeks or longer (Lin et al., 2025).
- Telemedicine significantly improves Constant-Murley score, Quick DASH score, pain, and range of motion in rotator cuff disorder patients compared to conventional treatment across 10 RCTs with 497 participants (Zhang et al., 2024).
- Initial in-person assessment is preferred when hands-on examination or manual therapy is clinically indicated. Telerehabilitation is most appropriate for supervised exercise delivery, home program progression, and follow-up care (Lin et al., 2025).
📋 When to Request OT, PT, or SLP Referral
Refer to Occupational Therapy (OT) when:
- Shoulder pain is limiting ADL performance, self-care, cooking, driving, or home management (Lafrance et al., 2022).
- Return to work is a goal and functional capacity evaluation, job demands analysis, or ergonomic worksite assessment is needed (Lafrance et al., 2022).
- Post-surgical ADL adaptation, sling management, or home modification guidance is required for safe discharge (Lafrance et al., 2022).
- Work-related shoulder pain involves physical or psychosocial occupational exposures requiring assessment and modification (Versloot et al., 2024).
Refer to Physical Therapy (PT) when:
- Any rotator cuff related shoulder pain is present. Exercise is first-line treatment and PT is the lead discipline (Desmeules et al., 2025).
- Shoulder strength deficits, range of motion restrictions, or movement dysfunction are limiting function. PT-led exercise is the evidence-based intervention (Zhang et al., 2026).
- Post-surgical rehabilitation is required following rotator cuff repair, shoulder replacement, or other shoulder procedures (Chen et al., 2024).
- In-person attendance is difficult. Telerehabilitation is an evidence-supported equivalent for many shoulder conditions (Lin et al., 2025).
Refer to Speech-Language Pathology (SLP) when:
- Cognitive-communication barriers limit the patient’s ability to engage with or follow shoulder rehabilitation instructions, particularly in neurological populations.
- Swallowing difficulties are present following cervical or shoulder surgery or in the context of neurological conditions with shoulder involvement.
- Pediatric shoulder pain in the context of CP or neurodevelopmental conditions requires communication-accessible rehabilitation.
Also See
- Back Pain — Rehabilitation for low back and neck pain that often co-occurs with shoulder conditions
- Osteoarthritis — Joint degeneration management relevant to glenohumeral OA and shoulder rehabilitation
- Activities of Daily Living — Adaptive strategies when shoulder pain limits daily independence
- Pain Management — Comprehensive OT, PT, and CBT approaches to chronic musculoskeletal pain
- Fall Prevention — Balance and strength programs relevant for older adults with shoulder and upper extremity involvement
- Home Modification and Safety — Adaptive strategies for managing shoulder conditions at home
- Stroke Recovery — Shoulder pain and hemiplegia management post-stroke
- Cancer Rehabilitation — Shoulder pain and upper limb rehabilitation following cancer treatment
References
Chen, Y., Meng, H., Li, Y., Zong, H., Yu, H., Liu, H., Lv, S., & Huai, L. (2024). The effect of rehabilitation time on functional recovery after arthroscopic rotator cuff repair: A systematic review and meta-analysis. PeerJ, 12, e17395. https://doi.org/10.7717/peerj.17395
Desmeules, F., Roy, J. S., Lafrance, S., Charron, M., Dube, M. O., Dupuis, F., Beneciuk, J. M., Grimes, J., Kim, H. M., Lamontagne, M., McCreesh, K., Shanley, E., Vukobrat, T., & Michener, L. A. (2025). Rotator cuff tendinopathy diagnosis, nonsurgical medical care, and rehabilitation: A clinical practice guideline. Journal of Orthopaedic & Sports Physical Therapy, 55(4), 235–274. https://doi.org/10.2519/jospt.2025.13182
Lafrance, S., Charron, M., Roy, J. S., Dyer, J. O., Fremont, P., Dionne, C. E., Macdermid, J. C., Tousignant, M., Rochette, A., Doiron-Cadrin, P., Lowry, V., Bureau, N., Lamontagne, M., Sandman, E., Coutu, M. F., Lavigne, P., & Desmeules, F. (2022). Diagnosing, managing, and supporting return to work of adults with rotator cuff disorders: A clinical practice guideline. Journal of Orthopaedic & Sports Physical Therapy, 52(10), 647–664. https://doi.org/10.2519/jospt.2022.11306
Lafrance, S., Charron, M., Dube, M. O., Desmeules, F., Roy, J. S., Juul-Kristensen, B., Kennedy, L., & McCreesh, K. (2024). The efficacy of exercise therapy for rotator cuff related shoulder pain according to the FITT principle: A systematic review with meta-analyses. Journal of Orthopaedic & Sports Physical Therapy, 54(8), 499–512. https://doi.org/10.2519/jospt.2024.12453
Lin, T. W., Yang, Y., Hong, H. Y., Zhou, X., Tung, T., Zheng, B., & Zhang, J. (2025). Effectiveness of telerehabilitation in non-operatively managed shoulder conditions: A systematic review and meta-analysis. BMC Musculoskeletal Disorders, 26, 614. https://doi.org/10.1186/s12891-025-08839-x
Lucas, J., van Doorn, P., Hegedus, E., Lewis, J., & van der Windt, D. (2022). A systematic review of the global prevalence and incidence of shoulder pain. BMC Musculoskeletal Disorders, 23, 1073. https://doi.org/10.1186/s12891-022-05973-8
Paraskevopoulos, E., Plakoutsis, G., Chronopoulos, E., & Papandreou, M. (2023). Effectiveness of combined program of manual therapy and exercise vs. exercise only in patients with rotator cuff related shoulder pain: A systematic review and meta-analysis. Sports Health: A Multidisciplinary Approach, 15(5), 727–735. https://doi.org/10.1177/19417381221136104
Versloot, A. H. C., Jackson, J. A., van Rijn, R. M., Elbers, R. G., Sogaard, K., Macri, E. M., Koes, B., Burdorf, A., Chiarotto, A., & Gerger, H. (2024). Physical and psychosocial work-related exposures and the occurrence of disorders of the shoulder: A systematic review update. Applied Ergonomics, 118, 104277. https://doi.org/10.1016/j.apergo.2024.104277
Zhang, B., Fang, Z., Nian, K., Sun, B., & Ji, B. (2024). The effects of telemedicine on rotator cuff related shoulder function and pain symptoms: A meta-analysis of randomized clinical trials. Journal of Orthopaedic Surgery and Research, 19, 478. https://doi.org/10.1186/s13018-024-04986-4
Zhang, B., Raguzzi, I. A., Dupuis, F., Gianola, S., Morgan-Daniel, J., Roy, J. S., & Pozzi, F. (2026). Addressing shoulder weakness in individuals with rotator cuff related shoulder pain: A systematic review with meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 56(2), 67–84. https://doi.org/10.2519/jospt.2025.13445
© TherapyTopics.com — All information is for educational purposes only and does not constitute medical or therapeutic advice. Consult a licensed therapist or physician for evaluation and treatment.